Fill Out a Valid Annual Physical Examination Template
Form Specs
| Fact Name | Description |
|---|---|
| Purpose | The Annual Physical Examination form is designed to gather comprehensive health information to ensure a thorough medical evaluation. |
| Required Information | Patients must provide personal details such as name, date of birth, and medical history to avoid unnecessary follow-up visits. |
| Immunization Records | Documentation of immunizations, including dates and types, is essential. This helps track vaccinations and ensure compliance with health guidelines. |
| Legal Compliance | In many states, the form complies with health regulations under laws such as the Affordable Care Act and HIPAA, ensuring patient privacy and rights. |
| Follow-Up Requirements | Patients may need to return for additional tests or consultations based on findings from the examination, ensuring ongoing health management. |
Dos and Don'ts
Filling out the Annual Physical Examination form can seem daunting, but it doesn't have to be. Here are some essential dos and don'ts to help you navigate the process smoothly.
- Do read the entire form carefully before you start filling it out. Understanding what information is required will save you time and effort.
- Don't leave any sections blank. Incomplete forms may lead to delays or additional visits.
- Do provide accurate and up-to-date information about your medical history, including any chronic conditions and medications.
- Don't forget to list all medications, including over-the-counter drugs and supplements. Omitting this information could affect your care.
- Do mention any allergies or sensitivities you have. This information is crucial for your safety during the examination.
- Don't rush through the form. Take your time to ensure that all details are correct and complete.
- Do ask for assistance if you have questions about any part of the form. It's better to clarify than to guess.
By following these guidelines, you can help ensure that your Annual Physical Examination goes as smoothly as possible. Your health is worth the effort!
Other PDF Documents
How to Make a Pdf Invoice - Gain confidence in your billing using our Free Invoice PDF Form.
The California Form REG 262 plays a crucial role in the transfer of ownership for vehicles and vessels in California. To ensure that the transfer process runs smoothly and in compliance with state laws, both buyers and sellers must properly complete this form, which should accompany the title or application for a duplicate title. For more detailed information about filling out the form, visit californiadocsonline.com/california-fotm-reg-262-form/.
P60 Form - The P45 helps employees maintain their tax code from one job to the next.
Common mistakes
-
Incomplete Personal Information: Failing to provide complete personal details, such as name, date of birth, and address, can lead to delays in processing the examination results.
-
Missing Medical History: Not including a comprehensive medical history summary or a list of chronic health problems can hinder the physician's ability to assess the patient's health accurately.
-
Incorrect Medication Details: Omitting current medications or providing inaccurate dosage and frequency information can result in unsafe medical recommendations.
-
Neglecting Allergies: Failing to disclose allergies or sensitivities can pose serious health risks, especially if medications or treatments are prescribed without this knowledge.
-
Ignoring Immunization Records: Not updating or accurately recording immunization dates can lead to unnecessary vaccinations or missed opportunities for preventive care.
-
Overlooking Follow-Up Recommendations: Disregarding recommendations for follow-up tests or evaluations can prevent timely diagnosis and treatment of potential health issues.
Documents used along the form
The Annual Physical Examination form is a crucial document that collects comprehensive health information from patients. It serves as a foundational element in evaluating an individual's overall health status. In addition to this form, several other documents are commonly utilized to enhance the assessment and management of a patient's health. Below are descriptions of four such documents that often accompany the Annual Physical Examination form.
- Medical History Form: This document provides a detailed account of a patient's past medical conditions, surgeries, allergies, and family health history. It helps healthcare providers understand potential risk factors and tailor their recommendations accordingly.
- Consent for Treatment Form: This form is essential for obtaining a patient's permission to proceed with medical examinations, procedures, or treatments. It ensures that patients are informed about the risks and benefits associated with the proposed care.
- Texas Dirt Bike Bill of Sale Form: To ensure thorough documentation of your sale, the necessary Texas dirt bike bill of sale steps provide important guidelines for a smooth transaction.
- Immunization Record: This document lists all vaccinations a patient has received, including dates and types of immunizations. It is vital for tracking immunization status and ensuring compliance with public health recommendations.
- Lab Test Requisition Form: Used to order specific laboratory tests, this form includes details about the tests required and any pertinent patient information. It facilitates communication between healthcare providers and laboratories, ensuring accurate test results.
These documents, when used in conjunction with the Annual Physical Examination form, create a comprehensive view of a patient's health. Together, they support informed decision-making and promote effective healthcare delivery.
Misconceptions
Misconceptions about the Annual Physical Examination form can lead to confusion and missed opportunities for important health assessments. Here are seven common misconceptions:
- It's only for sick people. Many believe that an annual physical is only necessary when feeling unwell. In reality, these exams are crucial for preventive care, allowing for early detection of potential health issues.
- All information is optional. Some think they can skip sections of the form. Completing all information is essential to provide a comprehensive view of your health and avoid return visits.
- Only doctors need to see the form. This form is also valuable for nurses and other healthcare providers. They use it to understand your medical history and current health status, ensuring coordinated care.
- Medications don't need to be listed if they're over-the-counter. Over-the-counter medications can interact with prescribed drugs. Always include all medications, whether prescription or over-the-counter, for accurate assessment.
- Immunizations are irrelevant if I'm healthy. Vaccinations are a critical part of preventive health care. Keeping immunizations up to date protects not only you but also those around you.
- Only women need GYN exams. While GYN exams are specifically for women, men also have their own necessary screenings, such as prostate exams. Both genders should be aware of their unique health needs.
- Once submitted, the form is done. It's important to review and update the form regularly. Health conditions and medications can change, and keeping the form current ensures your healthcare provider has the best information.
Understanding these misconceptions can help you make the most of your annual physical examination. Stay informed and proactive about your health.
Preview - Annual Physical Examination Form
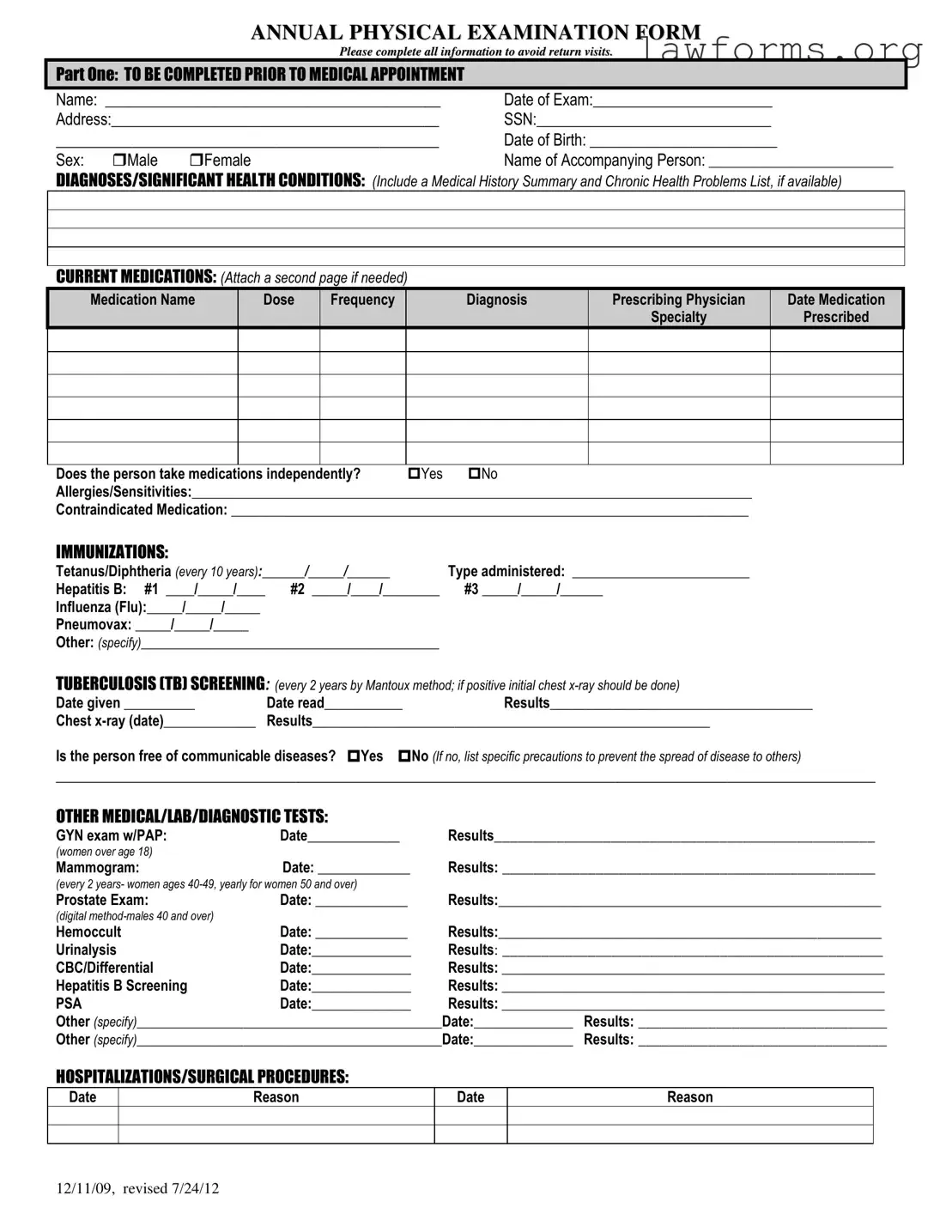
ANNUAL PHYSICAL EXAMINATION FORM
Please complete all information to avoid return visits.
PART ONE: TO BE COMPLETED PRIOR TO MEDICAL APPOINTMENT
Name: ___________________________________________ |
Date of Exam:_______________________ |
Address:__________________________________________ |
SSN:______________________________ |
_____________________________________________ |
Date of Birth: ________________________ |
||
Sex: |
Male |
Female |
Name of Accompanying Person: __________________________ |
DIAGNOSES/SIGNIFICANT HEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENT MEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
Yes |
No |
Allergies/Sensitivities:_______________________________________________________________________________ |
||
Contraindicated Medication: _________________________________________________________________________
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years):______/_____/______ |
Type administered: _________________________ |
|
Hepatitis B: #1 ____/_____/____ |
#2 _____/____/________ |
#3 _____/_____/______ |
Influenza (Flu):_____/_____/_____ |
|
|
Pneumovax: _____/_____/_____ |
|
|
Other: (specify)__________________________________________ |
|
|
TUBERCULOSIS (TB) SCREENING: (every 2 years by Mantoux method; if positive initial chest |
||
Date given __________ |
Date read___________ |
Results_____________________________________ |
Chest |
Results________________________________________________________ |
|
Is the person free of communicable diseases? Yes No (If no, list specific precautions to prevent the spread of disease to others)
_________________________________________________________________________________________________________
OTHER MEDICAL/LAB/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date_____________ |
Results_________________________________________________ |
(women over age 18) |
|
|
Mammogram: |
Date: _____________ |
Results: ________________________________________________ |
(every 2 years- women ages
Prostate Exam: |
Date: _____________ |
Results:______________________________________________________ |
|
(digital |
|
|
|
Hemoccult |
Date: _____________ |
Results:______________________________________________________ |
|
Urinalysis |
Date:______________ |
Results: _________________________________________________ |
|
CBC/Differential |
Date:______________ |
Results: ______________________________________________________ |
|
Hepatitis B Screening |
Date:______________ |
Results: ______________________________________________________ |
|
PSA |
Date:______________ |
Results: ______________________________________________________ |
|
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
HOSPITALIZATIONS/SURGICAL PROCEDURES:
Date
Reason
Date
Reason
12/11/09, revised 7/24/12

PART TWO: GENERAL PHYSICAL EXAMINATION
|
|
|
|
|
Please complete all information to avoid return visits. |
|
|
|
|
|
Blood Pressure:______ /_______ Pulse:_________ |
Respirations:_________ Temp:_________ Height:_________ |
Weight:_________ |
||||
|
|
EVALUATION OF SYSTEMS |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
System Name |
|
Normal Findings? |
Comments/Description |
|
||
|
|
Eyes |
|
Yes |
No |
|
|
|
|
|
Ears |
|
Yes |
No |
|
|
|
|
|
Nose |
|
Yes |
No |
|
|
|
|
|
Mouth/Throat |
|
Yes |
No |
|
|
|
|
|
Head/Face/Neck |
|
Yes |
No |
|
|
|
|
|
Breasts |
|
Yes |
No |
|
|
|
|
|
Lungs |
|
Yes |
No |
|
|
|
|
|
Cardiovascular |
|
Yes |
No |
|
|
|
|
|
Extremities |
|
Yes |
No |
|
|
|
|
|
Abdomen |
|
Yes |
No |
|
|
|
|
|
Gastrointestinal |
|
Yes |
No |
|
|
|
|
|
Musculoskeletal |
|
Yes |
No |
|
|
|
|
|
Integumentary |
|
Yes |
No |
|
|
|
|
|
Renal/Urinary |
|
Yes |
No |
|
|
|
|
|
Reproductive |
|
Yes |
No |
|
|
|
|
|
Lymphatic |
|
Yes |
No |
|
|
|
|
|
Endocrine |
|
Yes |
No |
|
|
|
|
|
Nervous System |
|
Yes |
No |
|
|
|
|
|
VISION SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
HEARING SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
ADDITIONAL COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical history summary reviewed? |
Yes |
No |
|
|
||
Medication added, changed, or deleted: (from this appointment)__________________________________________________________
Special medication considerations or side effects: ________________________________________________________________
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
___________________________________________________________________________________________________________
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)____________________
___________________________________________________________________________________________________________
Recommended diet and special instructions: ____________________________________________________________________
Information pertinent to diagnosis and treatment in case of emergency:
___________________________________________________________________________________________________________
Limitations or restrictions for activities (including work day, lifting, standing, and bending): No Yes (specify)
___________________________________________________________________________________________________________ |
|||
Does this person use adaptive equipment? |
No |
Yes (specify):________________________________________________ |
|
Change in health status from previous year? No |
Yes (specify):_________________________________________________ |
||
This individual is recommended for ICF/ID level of care? (see attached explanation) Yes |
No |
||
Specialty consults recommended? No |
Yes (specify):_________________________________________________________ |
||
Seizure Disorder present? No Yes (specify type):__________________________________ Date of Last Seizure: ______________ |
|||
________________________________ |
_______________________________ |
_________________ |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
Physician Address: _____________________________________________ |
Physician Phone Number: ____________________________ |
||
12/11/09, revised 7/24/12
Key takeaways
Completing the Annual Physical Examination form accurately is essential for ensuring a smooth medical appointment. Here are key takeaways to consider:
- Complete All Sections: Fill in every part of the form to prevent delays or the need for return visits.
- Provide Accurate Medical History: Include a summary of past diagnoses and chronic health issues to give the healthcare provider a comprehensive view of your health.
- List Current Medications: Document all medications you are taking, including dosages and prescribing physicians. Attach additional pages if necessary.
- Note Allergies: Clearly indicate any allergies or sensitivities to medications, as this information is crucial for safe treatment.
- Update Immunization Records: Provide dates and types of immunizations received, ensuring that your vaccination history is current.
- Communicable Diseases: Indicate whether you are free from communicable diseases and list any necessary precautions if applicable.
- Document Test Results: Include results from any recent medical tests, such as blood work or screenings, to assist in your evaluation.
- Provide Lifestyle Information: Share details about your lifestyle, including diet, exercise, and any adaptive equipment used, to help tailor health recommendations.
- Sign and Date: Ensure that the form is signed and dated by your physician, as this validates the information provided and confirms the examination.
Following these guidelines will help facilitate a thorough and effective annual physical examination, ultimately contributing to better health outcomes.
Similar forms
- Medical History Form: Similar to the Annual Physical Examination form, this document collects detailed information about a patient's past medical history, including previous illnesses, surgeries, and family health history.
- Consent for Treatment Form: This form, like the Annual Physical Examination form, requires patient information and ensures that the patient agrees to receive medical care and understands the procedures involved.
- Immunization Record: This document tracks vaccinations received, similar to the immunization section in the Annual Physical Examination form, which lists required immunizations and their dates.
- Medication Reconciliation Form: This form is used to review a patient’s current medications, much like the section in the Annual Physical Examination form that details current medications and their dosages.
- Health Risk Assessment: This document evaluates a patient's risk factors for various health conditions, paralleling the health condition inquiries found in the Annual Physical Examination form.
- Referral Form: Similar to the recommendations section in the Annual Physical Examination form, this document is used to refer patients to specialists for further evaluation or treatment.
- Lab Test Order Form: This form requests specific laboratory tests, akin to the diagnostic tests section in the Annual Physical Examination form, which lists tests and their results.
- Patient Registration Form: This initial form gathers basic patient information, similar to the demographic section in the Annual Physical Examination form that collects personal details.
- Quitclaim Deed Form: This legal document facilitates the transfer of property ownership in Ohio without guaranteeing the title's validity. For a comprehensive guide on completing this form, refer to Ohio PDF Forms, which offers essential resources for a smooth transaction.
- Follow-Up Care Plan: This document outlines recommendations for ongoing care, much like the health maintenance recommendations included in the Annual Physical Examination form.