Fill Out a Valid Medication Administration Record Sheet Template
Form Specs
| Fact Name | Description |
|---|---|
| Purpose | The Medication Administration Record (MAR) is used to document the administration of medications to consumers in various settings, ensuring accurate tracking and compliance with treatment plans. |
| Consumer Information | The MAR includes essential consumer details, such as name and attending physician, which are crucial for identifying the individual receiving medication. |
| Medication Hours | It provides a structured format for recording the time of medication administration, with designated hours for each day of the month. |
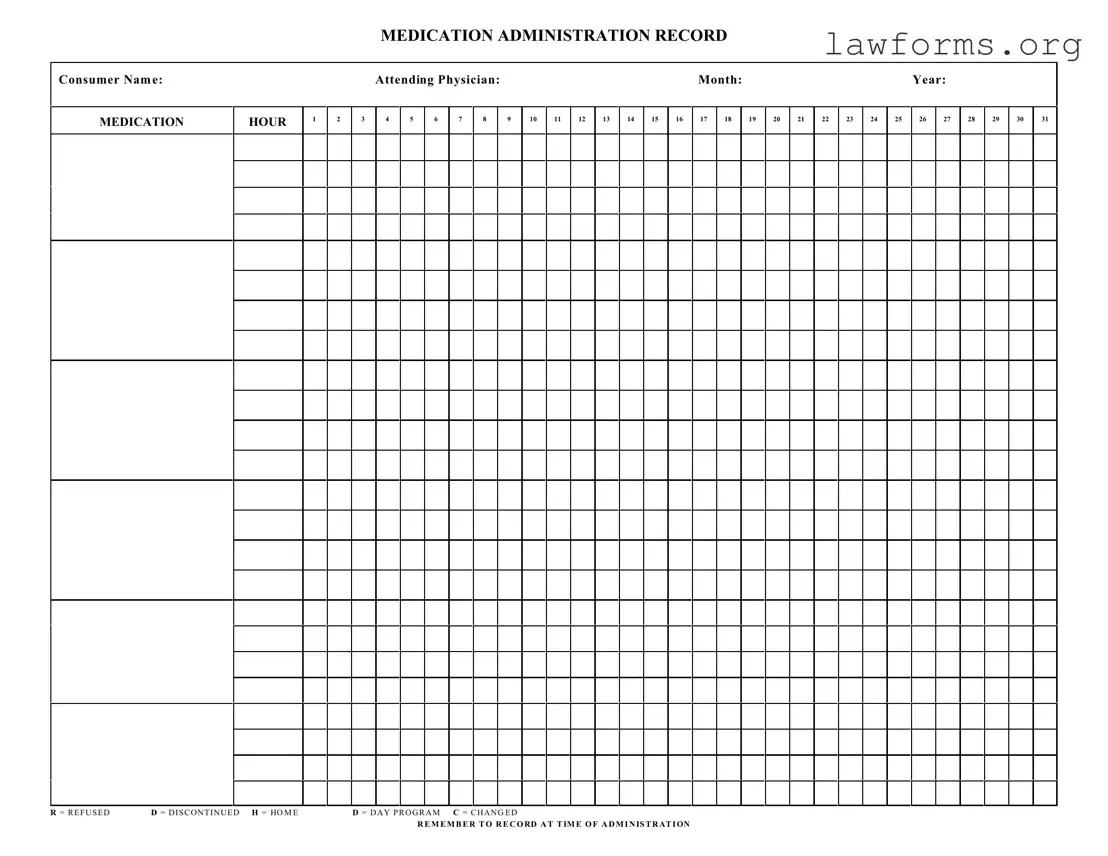
| Status Codes | The form includes specific codes (R, D, H, C) to indicate whether a medication was refused, discontinued, administered at home, or changed. |
| State Regulations | In many states, the use of MAR forms is governed by laws related to medication administration in healthcare facilities, ensuring compliance with state healthcare regulations. |
| Documentation Importance | Accurate and timely documentation on the MAR is vital for maintaining medication safety and providing a clear record for healthcare providers. |
Dos and Don'ts
When filling out the Medication Administration Record Sheet, it's essential to follow certain guidelines to ensure accuracy and compliance. Here’s a list of what to do and what to avoid:
- Do write clearly and legibly to prevent any misunderstandings.
- Do include the consumer's full name and the date of administration.
- Do record the time of administration accurately.
- Do mark any refusals or changes using the designated codes provided.
- Do ensure that the attending physician's name is noted on the form.
- Do review the completed form for any errors before submission.
- Don't leave any sections of the form blank; every part is important.
- Don't use abbreviations that are not listed on the form to avoid confusion.
- Don't alter any entries after they have been made; use a new entry for corrections.
- Don't forget to record any medications that were refused or discontinued.
- Don't submit the form without double-checking for accuracy.
- Don't share the form with unauthorized individuals; maintain confidentiality.
Other PDF Documents
Is It Too Late to Vaccinate My Cat - Keep a copy of this form for your pet’s health records.
To facilitate a smooth transfer and avoid potential disputes, it is advisable to utilize a reliable template when creating a Minnesota Bill of Sale form. You can find useful resources and templates at Formaid Org, which can help ensure that all necessary details are accurately captured, thereby safeguarding the interests of both parties involved in the transaction.
Konami Decklist - Your responsible documentation contributes to a successful event.
Common mistakes
-
Failing to include the consumer's name clearly at the top of the form. This can lead to confusion about who the medication is for.
-
Not recording the attending physician's name. This is essential for accountability and communication.
-
Overlooking the date when filling out the form. Accurate dates are critical for tracking medication administration.
-
Using incorrect medication hours. Ensure that the hours align with the prescribed schedule to avoid administration errors.
-
Neglecting to mark the appropriate codes such as R for refused or D for discontinued. This can cause significant issues in patient care.
-
Failing to record medication administration at the time of administration. This is crucial for maintaining accurate records.
-
Not updating the form when there is a change in medication. Changes must be documented immediately to ensure safety.
-
Using illegible handwriting when filling out the form. Clear writing is necessary for others to understand the information provided.
-
Forgetting to include initials or signatures of the person administering the medication. This is important for accountability and traceability.
Documents used along the form
The Medication Administration Record Sheet is an essential document used to track the administration of medications to consumers. It ensures that medications are given at the correct times and allows for proper documentation of any changes or refusals. Alongside this form, several other documents are commonly utilized to support medication management and care.
- Physician's Order Sheet: This document contains the specific instructions from a physician regarding the medications prescribed to a patient. It includes details such as dosage, frequency, and any special instructions, ensuring that all healthcare providers are on the same page.
- Medication Reconciliation Form: This form is used to compare a patient’s current medication list with the medications they were previously taking. It helps to identify any discrepancies, prevent medication errors, and ensure continuity of care during transitions between different healthcare settings.
- California LLC 12 Form: Ensures compliance for California limited liability companies, as detailed in the guidelines found here: https://californiadocsonline.com/california-llc-12-form.
- Incident Report Form: If there are any adverse reactions or medication errors, this form is completed to document the incident. It includes details about what occurred, the individuals involved, and any actions taken. This helps in improving safety and preventing future incidents.
- Patient Medication Education Record: This document is used to record the education provided to patients regarding their medications. It includes information on how to take the medication, potential side effects, and the importance of adherence, promoting better understanding and compliance.
These documents work together to create a comprehensive system for managing medications effectively. They help ensure that patients receive safe and appropriate care while also facilitating communication among healthcare providers.
Misconceptions
Understanding the Medication Administration Record Sheet (MARS) is crucial for ensuring proper medication management. However, several misconceptions can lead to confusion and errors. Here are five common misunderstandings:
- The MARS is only for nursing staff. Many believe that only nurses are responsible for filling out this form. In reality, anyone involved in medication administration, including caregivers and aides, should be familiar with it.
- It’s optional to record refused medications. Some think that noting a refused medication is not necessary. This is incorrect. Documenting refusals is essential for patient safety and for tracking medication compliance.
- All medications must be recorded at the same time. There’s a misconception that medications should be logged simultaneously. However, each medication should be recorded at the time of administration to ensure accuracy.
- Corrections can be made without following specific procedures. Many assume that they can simply cross out mistakes. In fact, proper procedures must be followed for corrections to maintain the integrity of the record.
- The MARS is only a legal document. While it serves as a legal record, it is also a vital tool for communication among healthcare providers. It ensures everyone is aware of the patient's medication regimen.
Addressing these misconceptions is essential for effective medication management and patient safety. Always prioritize accurate and timely documentation.
Preview - Medication Administration Record Sheet Form
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON
Key takeaways
Filling out and using the Medication Administration Record (MAR) Sheet is crucial for ensuring accurate medication management. Here are some key takeaways to keep in mind:
- Consumer Information: Always start by clearly writing the consumer's name at the top of the form. This ensures that the record is specific to the individual receiving medication.
- Physician Details: Include the attending physician's name. This helps in identifying who is responsible for prescribing the medications.
- Month and Year: Clearly indicate the month and year for the record. This is essential for tracking medication over time.
- Hourly Administration: The form provides slots for recording medication administration by hour. Be diligent in documenting the time each medication is given.
- Recording Refusals: If a consumer refuses medication, mark it with an "R" in the appropriate box. This is important for maintaining an accurate medication history.
- Discontinued Medications: If a medication is discontinued, indicate this with a "D." This prevents confusion about what medications are currently active.
- Changes in Medication: If there are any changes to the medication regimen, use a "C" to note this. Keeping track of changes is vital for ongoing care.
- Timely Recording: Remember to record the administration at the time it occurs. Delayed entries can lead to errors and mismanagement of the consumer's medication.
Similar forms
The Medication Administration Record Sheet form serves as a crucial tool in healthcare settings. It shares similarities with several other important documents. Below is a list of these documents and how they relate to the Medication Administration Record Sheet.
- Patient Medication List: This document outlines all medications prescribed to a patient, including dosages and administration times. Like the Medication Administration Record, it helps ensure that patients receive the correct medications at the right times.
- Divorce Settlement Agreement: This document outlines the terms of a divorce between parties, covering aspects such as property division and custody arrangements. For a comprehensive template, refer to Forms Washington.
- Medication Reconciliation Form: This form is used to compare a patient’s current medications with what is prescribed to prevent errors. Both documents aim to maintain accurate medication records to enhance patient safety.
- Nursing Notes: These notes document patient care and any observations made by nursing staff. Similar to the Medication Administration Record, they are essential for tracking patient progress and medication effects.
- Incident Report: This document records any medication errors or adverse reactions. Both the Incident Report and the Medication Administration Record are vital for identifying and addressing issues related to medication administration.
- Care Plan: A care plan outlines the overall treatment strategy for a patient, including medication management. Like the Medication Administration Record, it is integral to coordinating patient care and ensuring adherence to prescribed treatments.
- Medication Order Form: This form is used by healthcare providers to prescribe medications. Both this form and the Medication Administration Record are essential for ensuring that the correct medications are administered to patients.